Doctor on Demand: The Telehealth Innovation and Business Architecture
- Jun 6, 2017
- 9 min read
A meeting with a doctor usually lasts 7-15 minutes- that meeting takes almost half a patient day after adding commute times and wait times at the physician office. Consider that in 2015 adult patients in the US made 922.6 million visits to a physicians office of which over 53.2% were to a primary care physician. The most common diagnosed complaint - cough and essential hypertension. At the same time there were 125.7 million outpatient visits to a hospital. 93% of kids also had a contact with a health care professional. The loss of productivity is just staggering. Granted not all visits to an office are avoidable- but is there a way to avoid a certain percentage of these? Why does one need to travel to a physicians office to discuss the results of a blood test?
Healthcare organizations are looking to Telehealth to close the gaps in care delivery as well as a means to establish a more proactive brand and a dramatic improvement in patient experience. The UPMC advertisement on e-Dermatology, a Telehealth service speaks for itself.
Are Providers ready for the delivery of Virtual Care?
Change is never easy more so in Healthcare. There are footprints of Telehealth in most organizations, many still existing as science projects.

Payment reform and the outcome centric models are leading providers to consider Telehealth as a strategic construct of care delivery. Some providers have already augmented their virtual care offerings leveraging existing virtual care providers such as America Well or MD Live. Some perceive this as yet another siloed system and are pushing back and are building their own Virtual care capabilities. A recent study indicated that there are less than 50% primary care physicians in an
individual practice.
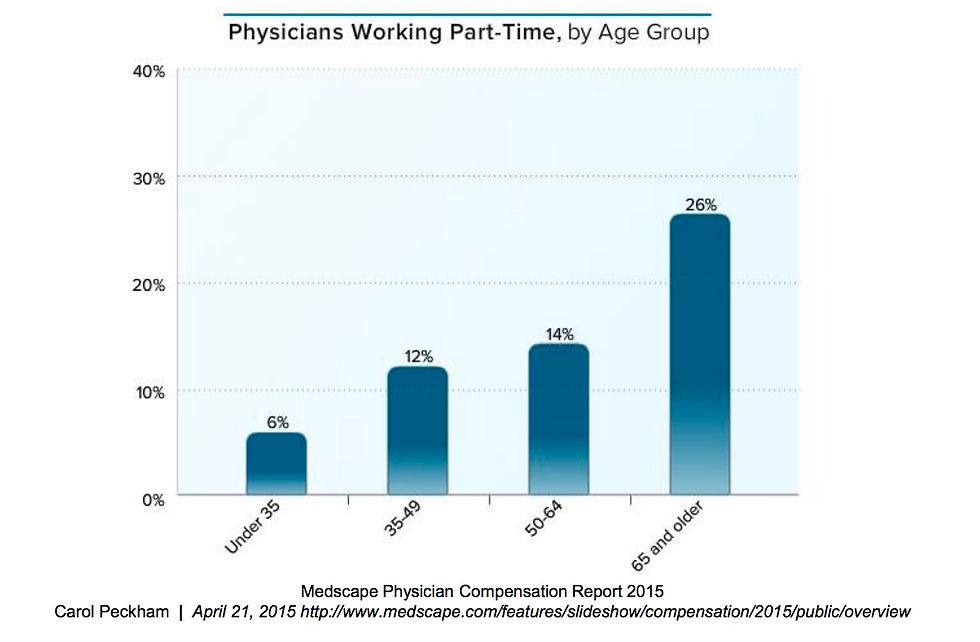
A Medscape report captured the physicians working part time by age group in the year 2015. There appears to be some evidence that physicians are available to work part time- a pool of the willing, that could be recruited to deliver virtual care services.
Is the market ready for Virtual care?
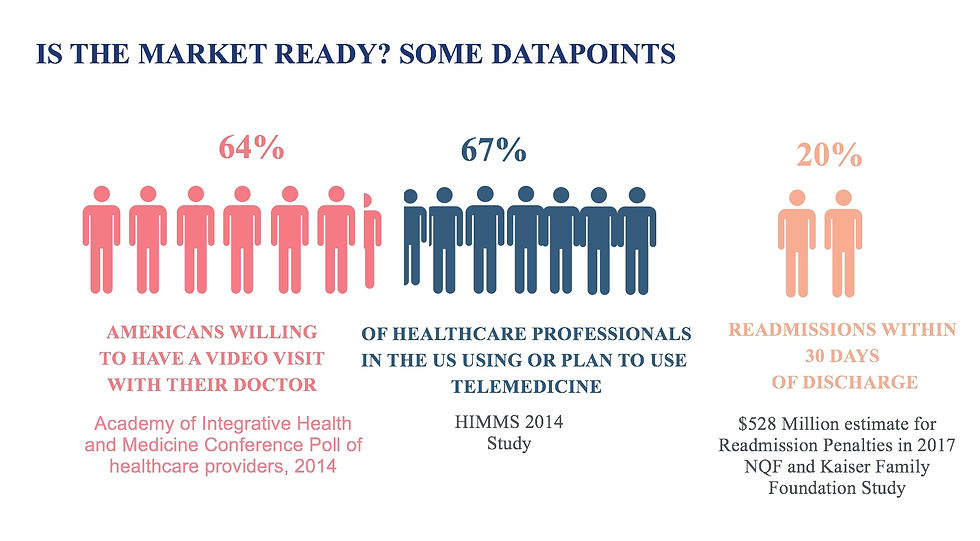
An Academy of Integrative Health took a poll on market acceptance of a video visit with their doctor. It found that 64% of Americans were willing to have a virtual visit. Over 67% of healthcare professionals either use or are planning to use Telemedicine. A big driver is cost containment.
Over 20% of patients were readmitted within 30 days; projected losses for readmission penalties for 2017 are $528 Million an increase over the penalties paid in 2016.
A perfect storm, that calls for a modified approach and a need to take care to the patient.
Of Business Models and Use Cases for Telehealth:
Telehealth by definition has a fairly broad context. Any service delivered virtually via text, E Mail, mobile applications or remote monitoring, even virtual patient education can be considered components of a Telehealth service.
There are two basic models:
Physician to physician or care teams
A Neurologist or cardiologist or pediatric specialist virtual consult with a provider- a hospitalist/intensivist/physician in an ED or ICU
A virtual nurse - nurse/physician consult
A provider virtual consult with a pharmacist or a radiologist or a pathologist
Physician or care teams to a patient
A physician/specialist consult with a patient
A nurse/care coordinator consult with a patient
A virtual patient education with a care team member
There are 3 primary delivery models:
Business to Consumer (B2C)
Largely a primary care model focused on responding to the retail-ization of healthcare services, direct patient access and support for common conditions and support to patients in urgent care settings
A chronic care management focus - coordinating care and managing CHF, COPD or diabetic patients. These services will be delivered to patient home (Home-healthcare), SNF , hospices etc.
A wellness and prevention service - mostly delivered through mobile Applications, augmented with virtual education
Patient monitoring at home
Business to Business (B2B)
Virtual clinical conferences where specialist discuss complicated conditions with referring physicians
A specialist providing services to physicians or care teams in another care setting such as a rural hospital
Care team collaboration- a visiting nurse consulting with a physician, specialist, social worker, or another nurse
Business to Business to Consumer
A specialist examining an acute patient at a primary care clinic or a rural hospital
A specialist supporting a remote intensivist in a rural ICU
Each of these models can be investigated to understand the use cases.
Behavioral health- Tele-psychiatry requires immersive video session
Tele-dermatology can be store and forward or require immersive video sessions
Tele-stroke - Immersive video as well as transmitting quality images (EKG)
Movement disorder - High quality video
Primary care - cough, cold etc. - An intelligent contact center construct for initial triage
Post acute care and consults - Cardiology, transplants, hip and knee replacement, bariatric surgery etc. - Medical device integration and high quality video
Patient education- Collaboration platforms
Virtual Clinical conference - high quality image transmission and video
Care coordination - Intelligent contact center
Requirements of a Telehealth program:
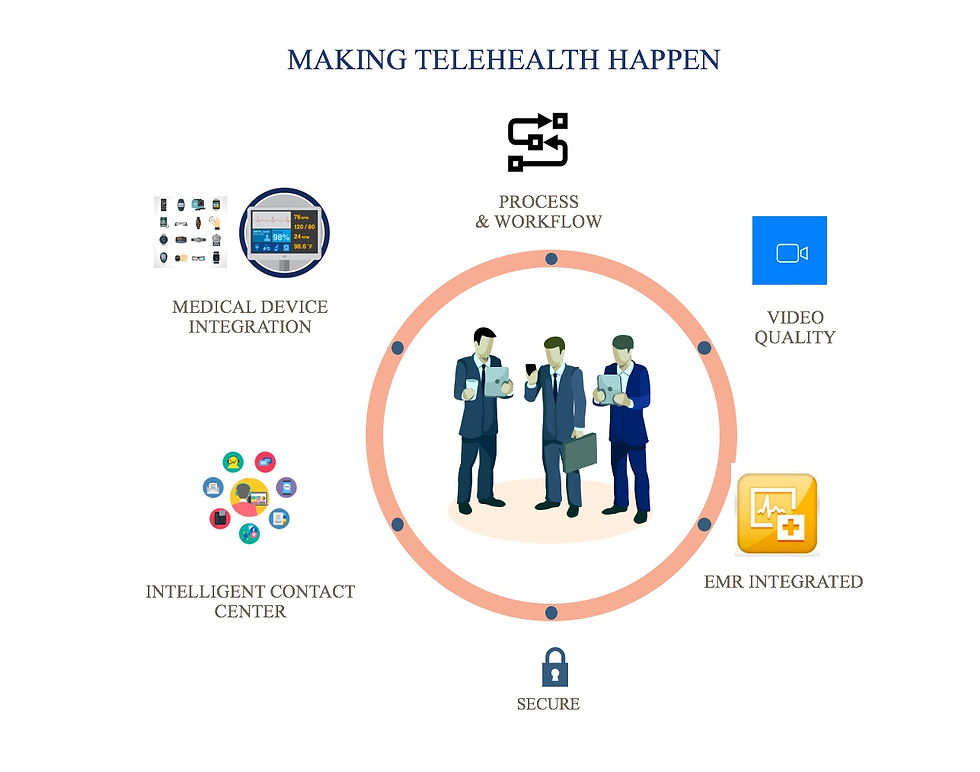
Four things to consider:
Technology - Largely dictated by the use case, however, some basic requirements:
Good quality video and an adequate bandwidth. Use cases will determine the basic minimum network speed and video quality needed
Provision omni channel - text and phone service along with the video.
Provision fall back approaches in case of channel failure
EMR Integrated Telehealth- A Telehealth service initiated through an EMR eliminates another siloed application and fragmented information. It eliminates the friction care teams feel trying to learn new solutions and managing sessions on multiple applications and screens.
Patients reach a system via the Contact Center. B2C models require a triage. An intelligent contact center integrated to the EMR allows intelligent routing of patient calls to the appropriate setting and Agent providing patient demographic and clinical context. Some B2C situations will start as ad-hoc calls, triaged at the Contact center and then converted to a scheduled call with a physician or specialist where appropriate
Some E&M visits especially post acute require the specialist to listen to the heart or lungs or examine a wound or the skin. Such use cases would require telemetry with devices such as Otoscopes, Welch-Allyns, Stethoscopes, Ultrasound or other equipments to transmit high fidelity signals/sounds/images from a remote patient over the network to the examining physician or specialist.
Security- Encrypted video and data transmission. HIPAA compliant storage of information.
Economics - Financial viability and sustainability have been a barrier for a faster adoption of Telehealth as an operational imperative. For many a provider Primary care has been a loss leader or marginally profitable. Each use case for Telehealth has a value associated and an outcome expectation. Not all use cases are alike in terms of the Impact to the business or the ease of implementation. Complexity of implementation can be impacted by a strategy misfit - a Specialty hospital will likely hire a Clinical specialist over a psychiatrist even though Tele-psychiatry as a use case may provide value. The absence of structure for Telehealth, Systemic misfits and technology silos, poor interoperability of data, poor process and untrained resources will impact the ease of implementation of a Telehealth use case. ROI models parse through the use cases segmenting them into cost optimizers, revenue generators, or drivers of operational efficiencies. Economic drivers for Telehealth include:
Revenue generation through broader patient outreach
Cost optimization- eliminating travel costs and increasing time with patients
Post acute care readmission management objective
Chronic care coordination - Elimination of unnecessary visit by chronic care patients
Operational efficiencies by bringing virtual specialists into care settings such as OR or ICU can improve patient care and flow as well as length of stay
Better brand image and increased patient satisfaction
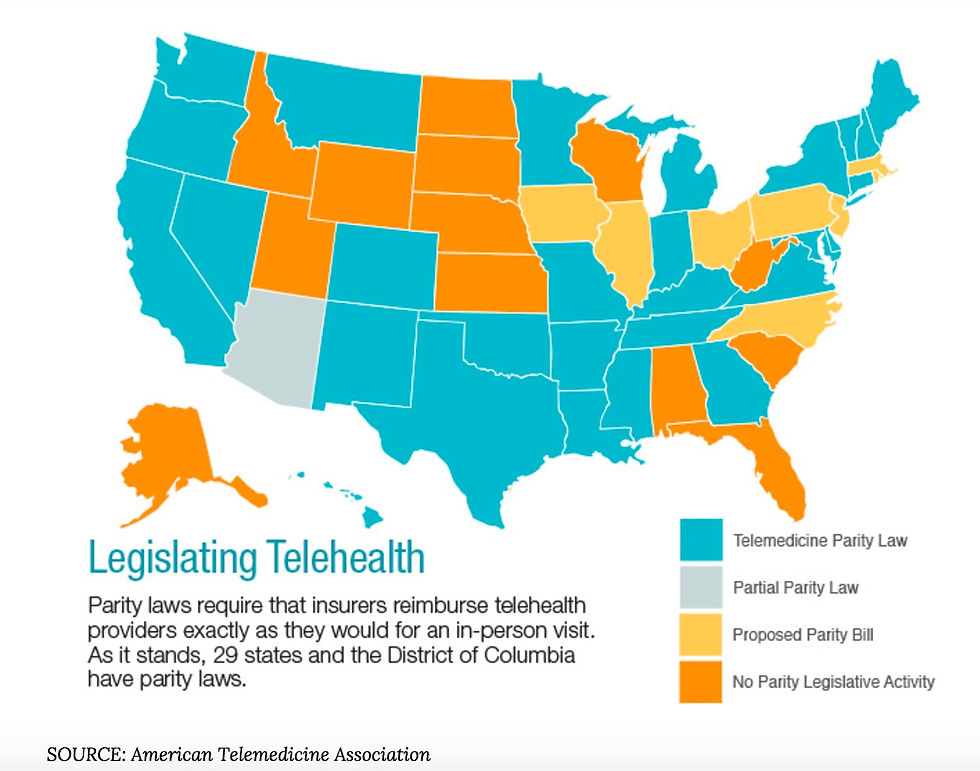
Telehealth reimbursement- Reimbursement in general is complex in Healthcare. For any one service a Provider has different charges: A Charge Master Rate- a charge that an uninsured patient or an International patient pays, a Medicare rate, A commercial insurer rate, a Blue rate, a usual customary reasonable rate (out of network), a Medicaid rate for reimbursement. The actual cost of the service is extremely difficult to extract. Telehealth adds another layer of reimbursement complexity. Medicaid reimbursement varies from State to State, medicare imposes certain restrictions on Telehealth. The CTel site http://ctel.org/expertise/reimbursement/ lists reimbursement policies for Telehealth by States in the US. Payment reform allows flexibility especially in Accountable Care organizations as it transfers some payment control to the organization. Forward thinking States have legislated parity laws for reimbursement of Telehealth services.
Process and Workflow- Healthcare is no stranger to the theories of path dependence. Processes built in the past, may no longer be relevant, yet constrain the implementation of new technologies. There are other drivers, legislation, regulation, licensing that also impacts Telehealth services. There has been little thought given to Telehealth processes that will be delivered at scale. Things to think about:
Licensure especially when practicing across State lines
Scheduling - B2C models tend to be ad-hoc in nature. A triage station in an Intelligent Contact center can convert the ad-hoc call into a scheduled call with an appropriate service level. B2B2C require scheduling resources at two sites, the provider and at the patient side in a clinic or other healthcare facility. If the service lines maintain their own calendar (and this is true with many a provider) scheduling can become a nightmare. Fortunately with IDN's using the same EMR based scheduling alleviates some of these scheduling nightmares. Patient portals provide visibility to patients on their upcoming visits and this should be the mechanism to inform patients of a Telehealth visit
Registration for new patients: B2C Models encourage new patients to request on-demand healthcare services. The Intelligent Contact Center Triage Agent should register the patient prior to scheduling the visit. That would require validation of Insurance, eligibility etc.
Workflows- A Telehealth workflow should be no different to a regular E&M workflow.
There should be a mechanism for the EMR system to electronically capture the reason for the visit, patient situation or concerns, transmission of vitals (from home or a remote clinic).
The patient should be kept waiting in a virtual wait room with indication of any delays in the start of the appointment.
Consults should take place over high definition Video. Some consults could be done using Audio or text based on the situation and the patient preference.
The physician should be able to e-prescribe any medication.
The Video consult should work integrated to the EMR system.
At the end of a session there should be a mechanism to schedule the follow up with appropriate notification. This would require a warm handover from the physician to a scheduling Agent/MA who would complete the scheduling process with the patient.
Workflows, especially in B2C models, should also manage patient queues allowing a pool of provider physicians to pick up patients from the queue.
Telehealth allows multi party conversations and the ability to bring in a language translator or a family member virtually in a Telehealth session would be an added bonus.
Workflows should allow for payment processing wherever possible, and the ability to collect co-pays at the time of the consult. That requires a deeper integration to internal payment processing systems. In some situations as in ACO's or with bundled payment mechanisms payment processing could be deferred or avoided as necessary.
Consent - Some States mandate a patient consent and mechanisms for e-Consent aligned to State requirements should be made
Quality - Patients should be provided a Survey to be filled after each session on their experience both with the consult as well as the technology. The organization should create a quality process that meets organizational, State , Federal, regulatory and accrediting requirements
Privacy and Confidentiality - Telehealth suites in a clinic should be sound proofed so that conversations in the suite remain in the suite. All information shared in the encounter/ recordings made should be securely captured and encrypted- the session itself should be encrypted.
Care provided via Telehealth should be no different from any of the standard requirements of an in person visits.
Identity -
There should be a mechanism to determine patient identity (at least 3 items- Name, date of birth, 4 digits of the Social Security) for every virtual consult.
At the same time and especially in B2C models patients should be able to validate provider identity (qualification, licensure, registration number)
The encounter should be recorded in the EMR and the patient provided a notification of the visit notes in the patient portal immediately after the consult.
The encounter patient record should contain patient demographic, healthcare facilities (such as ED's/ clinics/urgent care centers/acute facilities) near the patient, Emergency contacts and contact numbers, any local contacts in the event of an emergency.
Ensure technology works and is available during a consult
Check Audio and Video quality prior to every consult as well as the link to the patient site
Home Health:

Engagement@Home is Mercy Health's program to manage chronic patients at home- a program that has started to deliver promising outcomes.
Home health programs need careful considerations. Care coordinators or nurses will transparently be behind an Intelligent Contact Center. An integration of the Contact Center to the EMR will enable and empower a care team member as they receive information about the patient with context (clinical and demographic as well as healthcare resources near the patient) as the call comes through.
Omni channel collaboration will allow interaction with patients on their preferred channel. With enhanced integration care coordinators can co-browse and help patients navigate the Website, to fill forms, upload Insurance card images or virtual schedulers.
With a scaled robust Telehealth program that incorporates :
Patient monitoring and management
Relationship management
Care coordination and navigation
Patient education
Patient care
has the potential to transform services, improve clinical outcomes and reduce costs.
Comments